Anterior Cruciate Ligament (ACL) injuries remain a major clinical challenge requiring exhaustive functional evaluation to ensure recovery and prevent re-injury. Dynamic body surface scanning provides an innovative biomechanical approach by integrating morphological, kinematic, and functional metrics.
Dynamic morphology analysis enables objective quantification of structural variables (atrophy, edema) and functional variables (soft tissue deformation), improving precision in post-ACL assessment and supporting objective clinical decisions.
In this article, prepared by the IBV research team: Salvador Pitarch Corresa, Fermín Basso della Vedova, Paqui Peydro de Moya y Juan López Pascual. We explain the benefits of assessing this injury using 4D motion analysis technology such as MOVE4D, and we share the results of a use case based on this innovative technology.
Why functional ACL assessment is key in this type of injury
Structural integrity alone is not enough
Assessing only the integrity of the ligament reconstruction is not sufficient.
Dynamic evaluation through movement patterns is essential, as well as muscle monitoring to ensure a safe return to activity and reduce the risk of re-injury or joint degeneration.
There are examples in the literature [1,2] highlighting long-term morphological and physiological changes after ACL injury, including:
- Strength reduction
- Decreased cross-sectional area
- Loss of muscle volume
These deficits may persist even after surgical reconstruction.
Apparent gait symmetry may mask functional deficits
Several studies show that after ACL injury or reconstruction, gait kinematics may approach a nearly symmetrical pattern between the affected and contralateral limbs, particularly in advanced recovery stages.
However, this apparent normalization of joint kinematics does not imply full restoration of muscle function [3,4].
In other words:
- Movement may look normal
- Neuromuscular control may still be impaired
- Compensation strategies may persist
This creates a gap between clinical observation and real functional recovery.
Limitations of current clinical follow-up approaches
In routine clinical practice, follow-up after ACL reconstruction still relies mainly on time-based criteria to estimate recovery.
This is typically complemented by:
- Strength testing
- Functional performance knee tests
- Instrumental biomechanical assessments
While useful, these approaches do not always capture dynamic functional deficits.

Constraints of motion-capture technologies
Current motion-capture technologies used in ACL assessment include:
- 3D stereophotogrammetry
- Inertial Measurement Units (IMUs)
- Markerless systems
These systems provide joint kinematics data, but results may be influenced by technical limitations such as:
- Soft tissue artifact
- Sensor drift
- Sensor placement variability
- Task-dependent accuracy
- Population-specific variability
Challenges in muscle activity assessment
For muscle evaluation, surface electromyography (sEMG) is commonly used.
However, it presents known constraints:
- Crosstalk between adjacent muscles
- Sensitivity to electrode placement
Signal variability despite standardization guidelines
These factors can affect the reliability and accuracy of muscle function analysis.
Dynamic body surface scanning: MOVE4D, what it is and what it provides
This highlights the need for methodologies and evaluation systems that go beyond recording muscle activity or studying joint kinematics, incorporating morphological variables in both static and dynamic ways during functional movements.
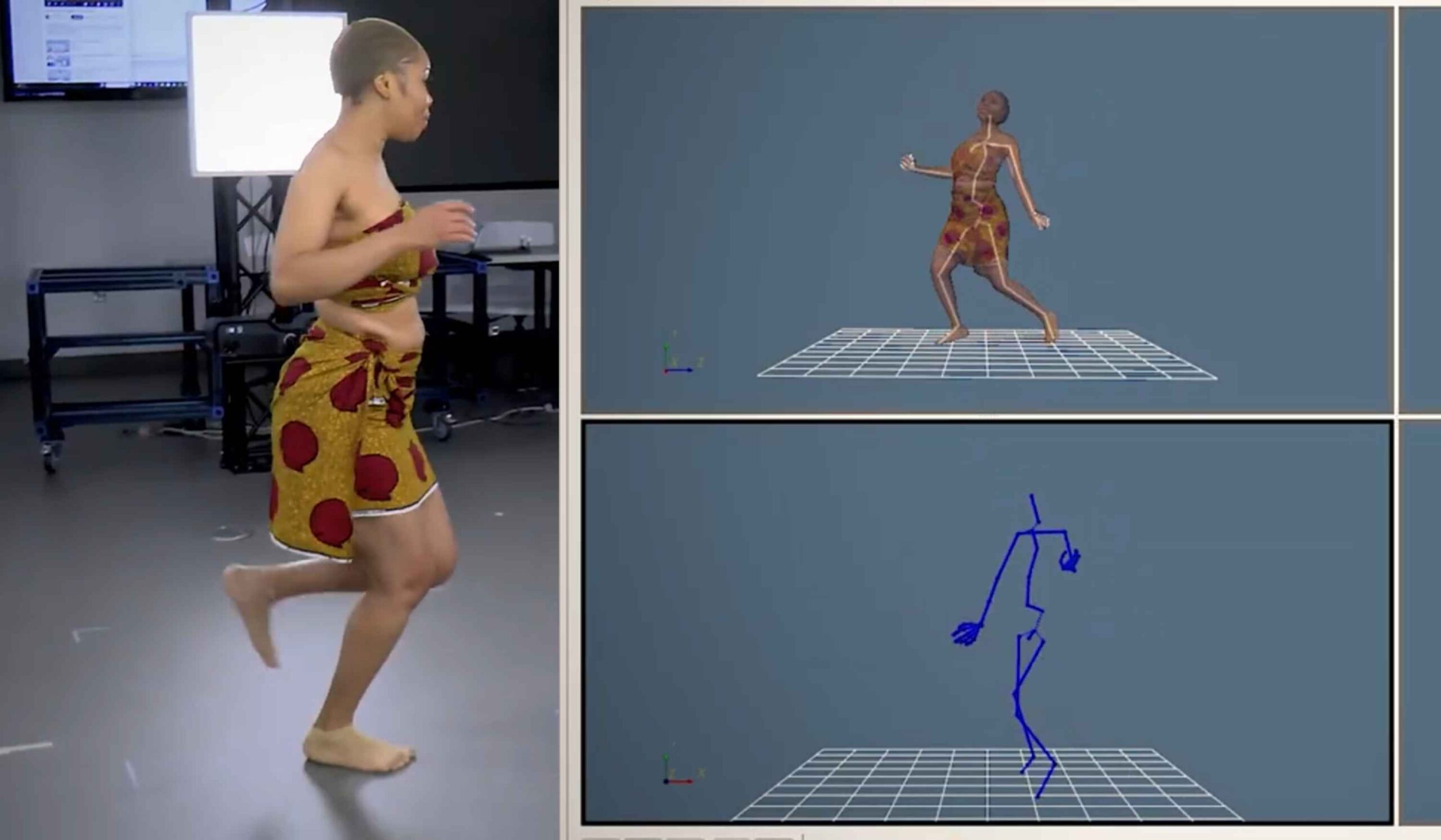
The MOVE4D dynamic body surface scanning system, combined with automated processing software, enables the generation of watertight and homologous digital human models. This homologous mesh, composed of 50k vertices, maintains a one-to-one correspondence throughout the entire temporal recording, thus allowing reproducible analysis of these metrics.
Main advantages of MOVE4D
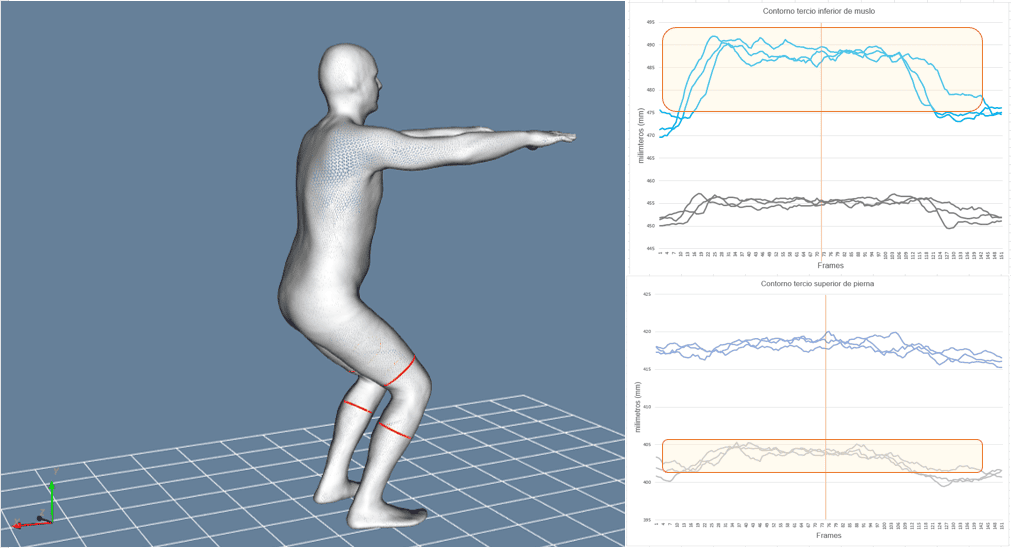
- It allows the visualization and quantification of changes in body geometry during movement, capturing the differences between static and dynamic postures.
- This technology can reveal how the body surface and its body measurements are altered with movement, which is valuable for understanding movement-related changes in body shape [5].
- MOVE4D offers direct and repeatable quantification of perimeters, areas, and volumes of body segments, making it possible to detect objective surface changes related to atrophy, edema, and muscle activity [6].
- Additionally, the information extracted from the homologous mesh enables reliable and accurate markerless calculation of joint kinematics [7,8].
- MOVE4D allows these metrics to be obtained in a simple, fast, and automated manner both statically and dynamically, during functional tasks or positions, representing a distinctive innovation.
This technology, in addition to obtaining joint kinematics without the need to instrument the subject, can provide another several advantages such as:
- Objectively quantifying muscle atrophy or the recovery of muscle volume.
- Analysing morphological symmetry between limbs during movement.
- Evaluating how the morphology of a body segment changes in specific phases of a functional movement.
The aim of this article is to describe the innovative contribution of dynamic surface scanning in the follow-up of ACL injuries, highlighting its potential to improve the accuracy of functional assessment.
You might be interested in this content: MOVE4D version 2.0: Greater precision, smarter automation, seamless Integration
Case study of ACL functional testing
This case study is presented involving a subject 3 month post-surgery for ACL and lateral meniscus in the right knee, who exhibits altered muscular trophism in the limb, primarily affecting weight-bearing movements.
Content development: materials. methods and methodology
A static study and assessments of gait and semi-squats were carried out using the MOVE4D system with the aim of:
- Obtaining joint kinematic data to determine movement functionality.
- Studying possible structural asymmetries through the static assessment of body segments.
- Identifying possible alterations in muscle function through the dynamic analysis of soft tissue behaviour.
The variables extracted from the study are:
- From the static assessment: the perimeter of the mid-thigh and the knee, in millimetres (mm).
- From the dynamic assessment: knee angles; perimeters of the distal third of the thigh and the upper third of the leg; and segmental volumes of the thigh and leg in litters (L) for each gait cycle analysis and semi-squat movement.
Results and interpretation
1. Kinematic Assessment
First, kinematic information was extracted through the mesh to help interpret the results of the morphological analysis.
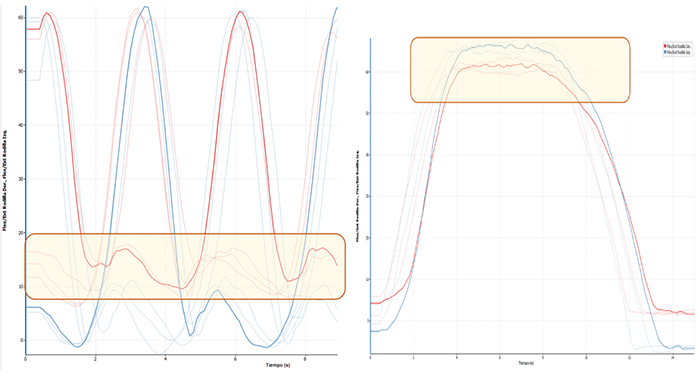
Figure 1. Joint kinematics of the operated right knee (red) and the healthy knee (blue) during gait (left) and semi-squat (right).
In general, gait functionality was normal at the kinematic level, with the exception of a slight flexion during the contact phase, which was maintained in the initial stance phase prior to swing. Additionally, during the semi-squat movement, a more or less symmetrical behaviour of the flexion angles was observed in the eccentric descent phase, with a difference of less than 5 degrees.
2. Static measurement: Morphological differences
The direct comparison between both limbs revealed clear structural asymmetries (Figure 2), specifically:
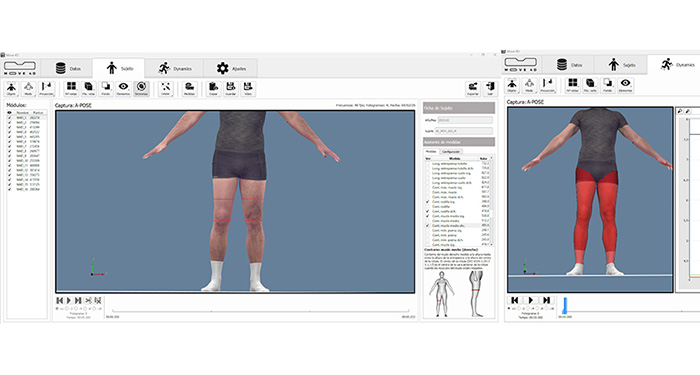
Figure 2. Static A-POSE position for calculating mid-thigh and knee perimeters (left) and thigh and leg volumes.
| Mid-thigh perimeter (mm) | Knee perimeter (mm) | Thigh volume (l) | Knee volume (l) | |
| Right (OL) | 493.5 | 410.8 | 7,63 | 4,10 |
| Left | 530.8 | 389.9 | 8 | 4,14 |
Table 1. Calculated values for mid-thigh and knee perimeters (left) and thigh and leg volumes (right) for both limbs in the static A-POSE position.
- A smaller perimeter and a reduction in volume were observed in the mid-thigh of the operated limb, consistent with muscle atrophy following the intervention and the period of load restriction.
- A larger perimeter was observed in the peripatellar region of the operated limb, consistent with possible residual oedema or inflammatory changes (Table 1).
These findings show a physiological asymmetry compared to thresholds established in large-scale anthropometric databases, such as CAESAR, where normal volumetric asymmetry in the thigh segment typically ranges between 3% and 5% [9]. In this case, the 4.6% volume deficit in dominant lower limb thigh, combined with a 3.7 cm difference in circumference, suggests a state of muscular atrophy. Consequently, this static assessment reflected a morphological asymmetry between limbs that provides an objective starting point for the subsequent dynamic functional interpretation.
3. Measurement of dynamic perimeters and volumes during gait
Below are the results related to leg and thigh perimeters during the gait cycle:
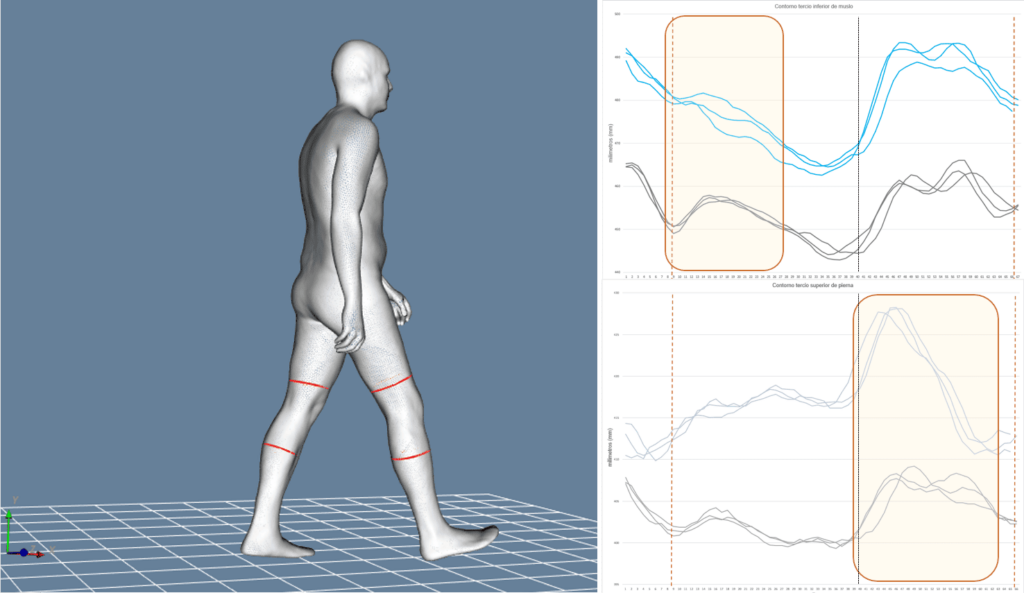
Figure 3. Dynamic perimeters of the lower third of the thigh (top right) and the upper third of the leg (bottom right) for both limbs during the gait cycle (blue: left / black: right).
| Maximum thigh perimeter (mm) | Minimum thigh perimeter (mm) | Thigh perimeter range (mm) | Maximum knee perimeter (mm) | Minimum knee perimeter (mm) | Knee perimeter range (mm) | |
| Right (OL) | 464.3 (1.5) | 443.8 (0.8) | 20.4 | 408.4 (0.7) | 399.6 (0.3) | 8.8 |
| Left | 491.8 (2.5) | 463.9 (1.2) | 27.9 | 428 (0.3) | 411.2 (0.8) | 16.8 |
Table 2. Mean values and standard deviation of maximum, minimum, and dynamic range perimeters of the lower third of the thigh and the upper third of the leg for both lower limbs during gait.
The following are the results related to leg and thigh volumes during the gait cycle:
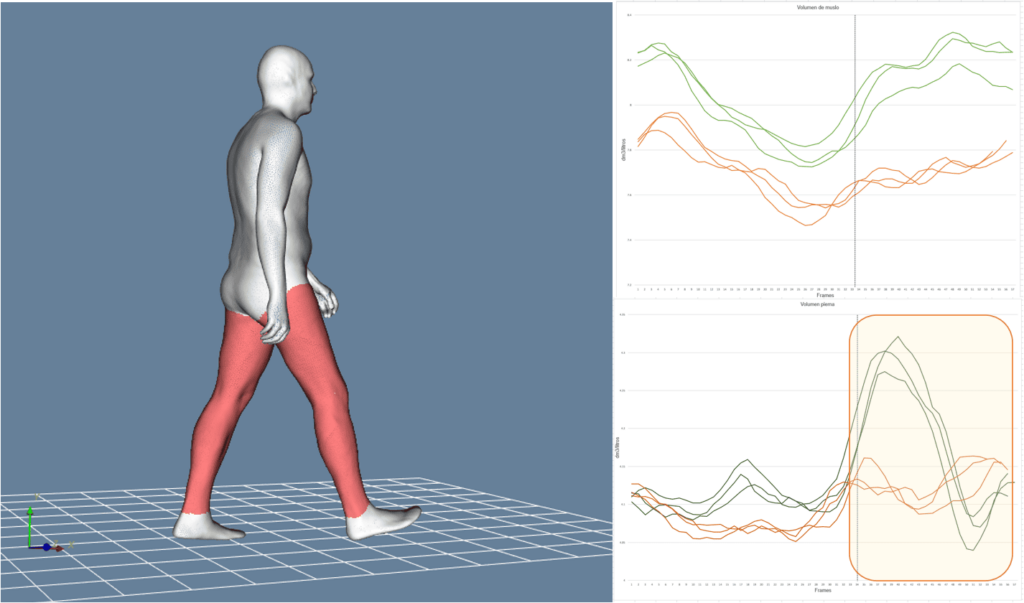
Figure 4. Dynamic thigh volumes (top right) and leg volumes (bottom right) for both limbs during gait cycles (green: left / orange: right).
| Maximum thigh volume (l) | Minimum thigh volume (l) | Thigh volume range (l) | Maximum knee volume (l) | Minimum knee volume (l) | Knee volume range (l) | |
| Right (OL) | 7.94 (0.04) | 7.52 (0.05) | 0.42 | 4.16 (0) | 4.06 (0.01) | 0.11 |
| Left | 8.28 (0.05) | 7.76 (0.05) | 0.52 | 4.30 (0.02) | 4.06 (0.02) | 0.24 |
Table 3. Mean values of maximums, minimums, range, and standard deviation of maximum and minimum thigh and leg volumes for both lower limbs during the gait cycle.
The gait assessment revealed significant morphological differences between both limbs, the most relevant being:
- A distinct deformation pattern was observed between the two limbs for both thigh and leg perimeter during the initial loading and stance phases, as well as the swing phase (Figure 3).
- The perimeter amplitude was generally smaller in the operated limb compared to the healthy one (Table 2).
- Significant differences were observed in leg volume during the take-off and swing phases of the injured limb compared with the contralateral limb (Figure 4).
- The magnitude of the differences in dynamic thigh and leg perimeters and volumes during the execution of the movement remained in the same proportion as those observed in the static assessment (Tables 2 and 3).
- The registers are highly repeatable for perimeters and volumes.
The findings obtained from the morphological analysis described above suggest a reduced involvement of the injured limb in controlling the stance and take-off phases, consistent with the kinematic behaviour previously observed.
The overall difference indicates that, although gait was functional, soft tissue dynamics are not yet normalized compared to the healthy limb.
4. Measurement of dynamic circumferences and volumes during the semi-squat gesture.
The following are the results related to leg and thigh perimeters during the semi-squat cycle:
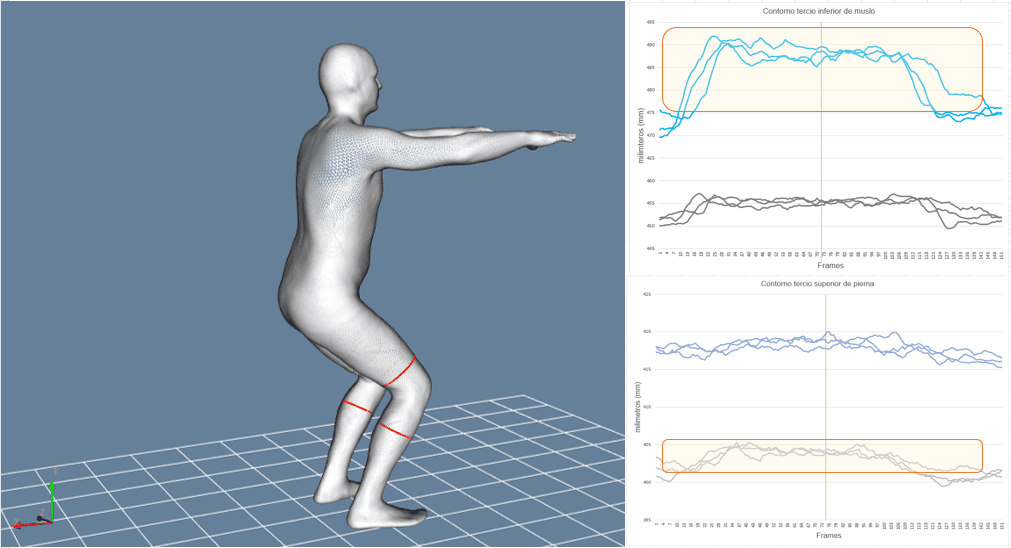
Figure 5. Dynamic perimeters of the lower third of the thigh (top right) and the upper third of the leg (bottom right) for both limbs during the semi-squat (blue: left / black: right).
| Maximum thigh perimeter (mm) | Minimum thigh perimeter (mm) | Thigh range (mm) | Maximum knee perimeter (mm) | Minimum knee perimeter (mm) | Knee range (mm) | |
|---|---|---|---|---|---|---|
| Right (OL) | 456.5 (0.47) | 450.9 (1.3) | 5.52 | 403.8 (0.42) | 400.2 (0.85) | 3.6 |
| Left | 488.8 (0.8) | 474.0 (0.85) | 14.78 | 418.9 (0.96) | 416 (0.8) | 2.87 |
Table 4. Mean values of maximum perimeter, minimum perimeter, amplitude, and standard deviation of the dynamic perimeters of the lower third of the thigh and the upper third of the leg for both lower limbs during the semi-squat.
Below are the results related to leg and thigh volumes during the semi-squat cycle:
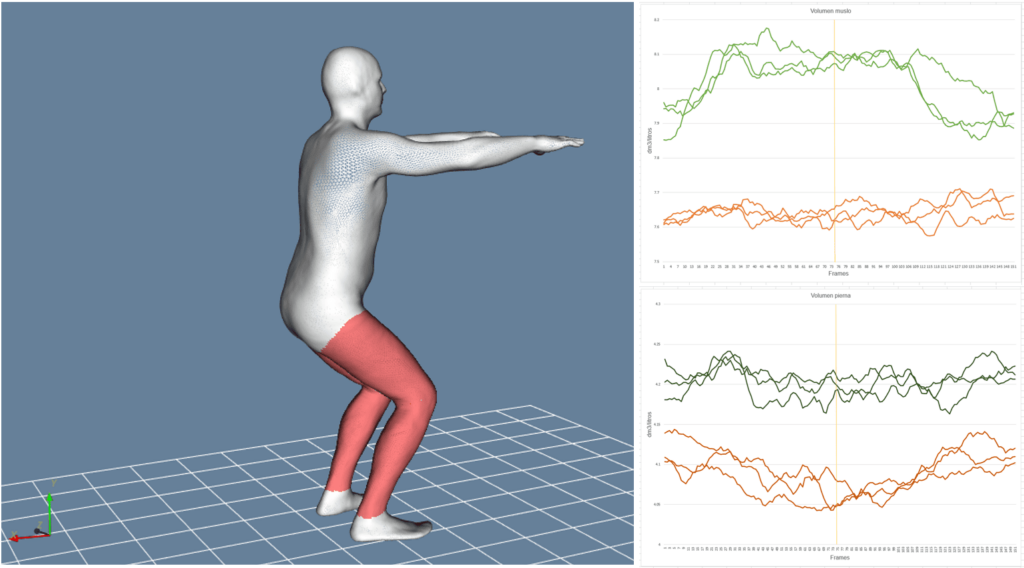
Figure 6. Dynamic thigh volumes (top right) and leg volumes (bottom right) for both limbs during the semi-squat (green: left / orange: right).
| Maximum thigh volume (l) | Minimum thigh volume (l) | Thigh volume range (l) | Maximum knee volume (l) | Minimum knee volume (l) | Knee volume range (l) | |
| Right (OL) | 7.69 (0.03) | 7.60 (0.02) | 0.09 | 4.12 (0.02) | 4.06 (0.01) | 0.06 |
| Left | 8.218 (0) | 7.88 (0.02) | 0.23 | 4.23 (0.01) | 4.17 (0.01) | 0.05 |
Table 5. Mean values of maximums, minimums, range, and standard deviation of maximum and minimum thigh and leg volumes for both lower limbs during the semi-squat cycle.
The comparison of both limbs during the semi-squat movement made it possible to identify more clearly the differences in muscle demand and postural control, highlighting:
- A deformation pattern of the injured limb different from that of the healthy limb was observed, both in perimeter values and in thigh and leg volumes (Tables 4 and 5).
These differences may indicate an increased load and activity in the thigh of the healthy side during the eccentric phase of the movement, as well as stabilization through the injured leg (Figures 5 and 6), even when the kinematic knee flexion values or rates do not differ by more than 5 degrees.
This comparison showed that functional deficits were more noticeable in tasks with high eccentric demand and load, where the injured limb does not reproduce the same loading pattern as the healthy one.
5. Assessment overall summary
The analysis of this case study highlights several key findings:
- The structural assessment shows that the injured limb presents greater atrophy and morphological changes that are not present in the healthy side, common finding in the 3-month post-ACL reconstruction phase.
- In the assessment of gait function, differences in morphology and magnitude of both perimeters and volumes are observed in the thigh and leg of the injured limb, which may represent functional deficits such as compensatory strategies.
- During the execution of the semi-squat movement, the differences between limbs become amplified, revealing reduced eccentric capacity and protective strategies in the injured limb that are not present in the healthy limb.
Overall, the morphological analysis reveals persistent differences in soft-tissue volume and deformation, aligned with altered muscle function and supported by kinematic data.
Bilateral comparison makes it possible to identify structural and functional deficits that may persist for months or even years after surgery.
These findings reinforce existing evidence:
- Symmetrical gait does not guarantee full muscle recovery.
- Muscle morphology directly influences performance in high-demand tasks such as descents or accelerations.
In this context, emerging technologies such as 4D dynamic body surface scanning provide new opportunities for functional ACL testing or evaluation.
By quantifying soft-tissue deformation, these systems can:
- Detect asymmetries not visible in standard gait analysis.
- Offer insight into real neuromuscular status.
- Complement traditional clinical and biomechanical assessments.
Integrating these technologies may improve diagnostic accuracy and support better decisions on functional progression and safe return to sport or work.

Key ideas and conclusions
Dynamic surface analysis expands ACL follow-up by integrating morphological, functional, and kinematic data in a single, markerless workflow. Its main advantages are fast acquisition, minimal preparation, repeatability, and greater objectivity.
This technology allows clinicians to:
- Quantifying the recovery of quadriceps and leg muscle volume by comparing the injured and non-injured sides.
- Detecting functional asymmetries in contraction during gait or load-bearing exercises.
- Objectively measuring joint mobility in functional exercises without the need for markers.
- Recording longitudinal progression quickly and reproducibly across different phases of rehabilitation.
In summary, the dynamic scanner emerges as an objective, non-invasive, and easy-to-use tool capable of providing a global perspective through the study of the dynamic behaviour of the body surface.
References
[1] Dutaillis B, Maniar N, Opar DA, Hickey JT, Timmins RG. Lower Limb Muscle Size after Anterior Cruciate Ligament Injury: A Systematic Review and Meta-Analysis. Sports Med. 2021 Jun;51(6):1209-1226. doi: 10.1007/s40279-020-01419-0.
[2] Owen, M.K., Richardson, L., Johnson, D.L. et al. Alterations in whole muscle quality and physiological cross-sectional area measured with quantitative MRI following ACL injury. J Transl Med 23, 79 (2025). https://doi.org/10.1186/s12967-024-05980-4.
[3] Lewek, M., Rudolph, K., Axe, M., & Snyder-Mackler, L. (2002). Quadriceps femoris muscle weakness and articulation during gait after ACL reconstruction. Clinical Biomechanics, 17(8), 604–614.
[4] Hart, H. F., Culvenor, A. G., Collins, N. J., & Crossley, K. M. (2016). Knee kinematics and joint moments during gait following anterior cruciate ligament reconstruction: A systematic review and meta-analysis. British Journal of Sports Medicine, 50(10), 597–612.
[5] Klepser A, Morlock S. 4D Scanning – Dynamic View on Body Measurements. 2020 Sep. 21;1(1):30-8. https://doi.org/10.25367/cdatp.2020.1.p30-38.
[6] Basso Della-Vedova, F., De Rosario, H., Belda-Lois, JM., Porcar-Seder, R. (2024). Deformation of Skin in 4D Scans as an Indicator of Muscular Activity Compared to EMG in Biceps Contraction. In: Pons, J.L., Tornero, J., Akay, M. (eds) Converging Clinical and Engineering Research on Neurorehabilitation V. ICNR 2024. Biosystems & Biorobotics, vol 32. Springer, Cham. https://doi.org/10.1007/978-3-031-77584-0_69.
[7] Ana V. Ruescas-Nicolau, Helios De Rosario, Eduardo Parrilla Bernabé, M.-Carmen Juan, Positioning errors of anatomical landmarks identified by fixed vertices in homologous meshes, Gait & Posture, Volume 108, 2024, Pages 215-221, ISSN 0966-6362, https://doi.org/10.1016/j.gaitpost.2023.11.024.
[8] Ana V. Ruescas Nicolau, Helios De Rosario, Fermín Basso Della-Vedova, Eduardo Parrilla Bernabé, M.-Carmen Juan, Juan López-Pascual, Accuracy of a 3D temporal scanning system for gait analysis: Comparative with a marker-based photogrammetry system, Gait & Posture, Volume 97, 2022, Pages 28-34, ISSN 0966-6362, https://doi.org/10.1016/j.gaitpost.2022.07.001.